Peptic Ulcers And Helicobacter Pylori
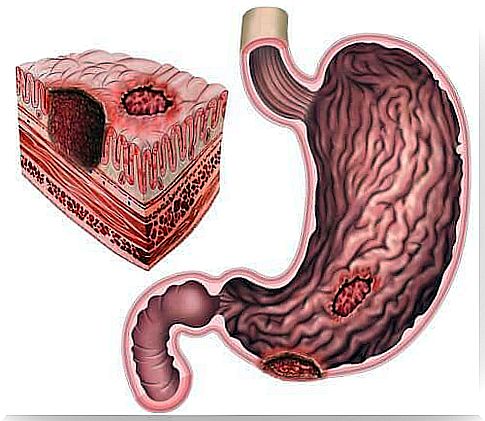
Peptic ulcers are lesions with loss of substance from the gastroduodenal mucosa. Although their incidence is decreasing, they continue to affect a large part of the population.
The Helicobacter pylori is found in over 90% of cases of peptic ulcer. These are a type of bacteria that cause stomach infections.
It can be found in approximately two-thirds of the world’s population. It is possible that it is transmitted through contaminated food and water.
Causes of peptic ulcers

Most ulcers are caused by an imbalance between aggressive and defensive agents in the gastroduodenal mucosa. This imbalance is secondary to Helicobacter pylori infection or consumption of non-steroidal anti-inflammatory drugs (NSAIDs).
In cases of peptic ulcer with Helicobacter, eradication of the bacteria will reduce recurrences. However, only 10 to 20% of people infected with Helicobacter pylori will develop a peptic ulcer.
When there is a chronic use of NSAIDs, 50% of these people have superficial gastric lesions. In addition, ulcers in these cases are often asymptomatic.
Risk factors for peptic ulcer in people who use NSAIDs are:
- peptic ulcer history
- Age: over 60 years old
- Use of anticoagulants or corticosteroids.
- High doses of NSAIDs.
- Infection with Helicobacter pylori.
Although smoking seems to negatively influence the healing of peptic ulcers, there are no studies showing that smoking, stress and diet are factors capable of triggering peptic ulcers.
Symptoms and Diagnosis of Peptic Ulcers
Most people with ulcers have symptoms of dyspepsia. The pattern of dyspepsia symptoms already guides the diagnosis of ulcer. Symptoms include epigastric pain on an empty stomach, which disappears with food intake or the use of antacids.
For diagnosis, it is important to have information about lifestyle, pharmacological treatments, and personal history of ulcer or Helicobacter pylori infection.
In some people, the ulcer can coexist with gastroesophageal reflux disease. This can make diagnosis difficult. The most sensitive and specific test to confirm the existence of an ulcer is upper digestive endoscopy (gastroscopy).
Treatment of peptic ulcers

The goal of treatment is to relieve symptoms, heal ulcers and, ultimately, prevent complications. In addition, it is recommended to follow some hygienic-food measures, such as:
- Avoid using NSAIDs.
- Stop eating foods and drinks that cause symptoms.
- Do not smoke, as tobacco delays ulcer healing and increases recurrences.
antisecretory treatment
Currently, the inhibitors of proton pump (PPIs) are the drugs that affect higher rates of healing of the mucosa.
They must be taken before meals. Also, there are studies that show greater effectiveness if they are taken in the morning rather than at the end of the day.
Proton pump inhibitor drugs take 3 to 5 days to reach maximum effect. However, there is variability in the clinical response due to hepatic drug metabolism.
The duration of peptic ulcer treatment depends on its location. In the case of duodenal ulcer, it lasts 4 weeks, while gastric ulcer takes between 6 and 8 weeks.
Eradication of Helicobacter pylori
Eradication of the bacteria causes the ulcer to heal. In addition, long-term ulcerative complications are also reduced.
The first-line eradication treatment is to administer a PPI and antibiotics (clarithromycin, amoxicillin, and metronidazole) for at least ten days.
In patients allergic to penicillin, PPI, clarithromycin, and metronidazole are used as a first choice for at least 10 days.
Recommendations for the use of NSAIDs
When there are risk factors for peptic ulcer, before taking NSAIDs, it is recommended to consider the following advice:
- Review the indication : if the effect we are looking for is analgesia or a decrease in fever, it is more appropriate to take paracetamol.
- Always use the lowest effective dose of NSAIDs and, in addition, the least toxic.
- Finally, anticoagulants and corticosteroids together.